Artificial intelligence in radiology — use cases and trends
AI radiology is among the most production-mature healthcare AI subfields. Where it ships today, the FDA-cleared tools in clinical use, and the implementation discipline that separates production deployments from pilots.

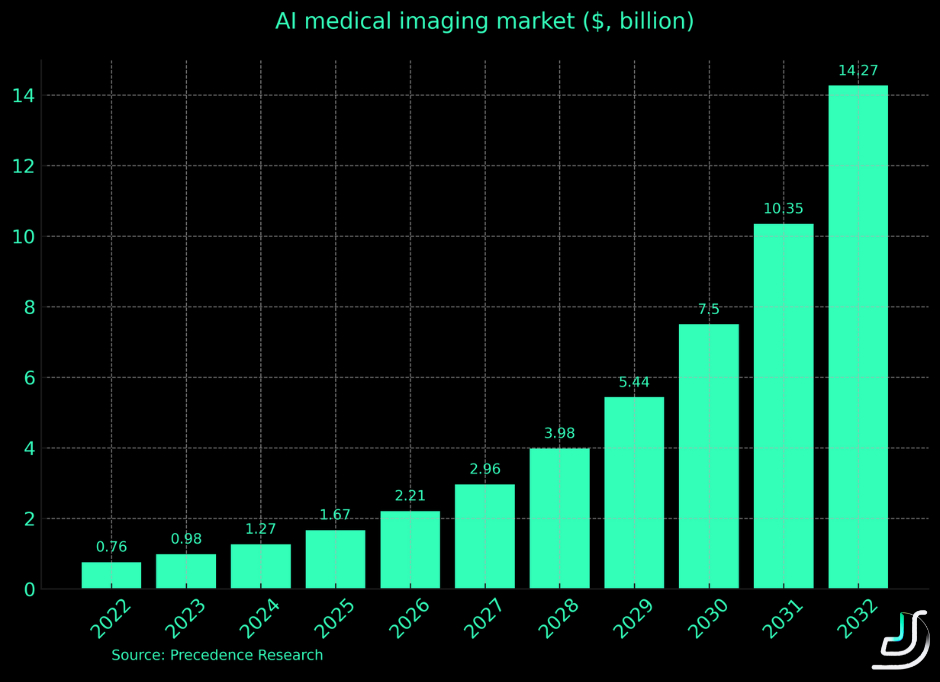
AI radiology is among the most production-mature subfields in healthcare AI. Unlike GenAI for clinical decision-making — where regulatory clarity is still emerging — radiology AI has FDA-cleared tools in active clinical use, peer-reviewed studies validating accuracy on bounded tasks, and measurable improvements in radiologist productivity. The market reflects the maturity: AI in medical imaging was $0.98B in 2023, projected to exceed $14B by 2032.
This article maps where AI is genuinely working in radiology today, with public reference deployments, and the implementation challenges teams plan for. For broader healthcare AI cost framing, see assessing the cost of implementing AI in healthcare. For deeper treatment of healthcare AI agents (which often pair with radiology imaging), see how AI agents transform the healthcare sector.
The pressure driving AI radiology adoption
Even before the pandemic, 45% of radiologists experienced burnout. Daily scan volume per radiologist routinely exceeds 100. Administrative burden compounds the problem. AI radiology addresses these pressures with measurable productivity gains:
- GE Healthcare reports AI image reconstruction enables scanning 35 patients per day vs. 25 — a 40% throughput increase
- Swedish researchers reduced radiologist mammogram reading load by 44% using AI-assisted screening
- AI-augmented mammography improves cancer detection rate by 20% with comparable false-positive rates
These aren't pilot results — they're production deployments measuring real workflow impact in clinical settings.
What AI radiology actually does
Three AI subtypes deliver value in radiology workflows:
- Deep learning and computer vision analyze medical images for preliminary diagnosis, abnormality detection, and segmentation. Modern systems hit 95%+ accuracy on bounded tasks (specific fracture types, specific cancer screenings). For deeper treatment of CV in healthcare and beyond, see computer vision applications across industries.
- Computer-aided detection (CAD) — the original radiology AI category. Traditional CAD uses predefined algorithms; modern CAD uses deep learning for autonomous learning and broader application surface.
- Generative AI — synthesizes medical images, generates radiology reports, augments training datasets. The newest application area, with regulatory pathway still emerging.
Four primary benefits driving deployment
Early-stage disease detection. AI sees patterns radiologists miss. A Boston research team's lung cancer prediction tool reaches 86–94% accuracy for next-year cancer development risk. Earlier detection translates directly to better outcomes and lower treatment costs.
Improved patient outcomes via screening augmentation. AI as the second reader on mammograms, CT scans, MRI sequences. The Swedish 20% detection rate improvement is one of many published studies showing measurable accuracy gains.
Radiologist workload reduction. AI handles the high-volume routine cases, freeing radiologists for complex interpretation and patient consultation. HOPPR's Grace foundation model supports radiologists in scan reading, transcribes comments, and drafts radiology reports.
Education and research acceleration. GenAI synthesizes realistic medical scans for training datasets, simulates disease progression scenarios for medical education, generates annotated training data for new AI model development.
Five production use case categories
1. Brain tumor classification
Brain cancer is the 10th leading cause of death in the US. Pre-operative tumor classification was historically a leap of faith — surgeons often didn't know tumor type until biopsy results came back days later. AI is changing this.
Reference deployments:
- UMC Utrecht's intra-operative brain tumor classification tool studies tumor DNA in real-time during surgery, identifying type and subtype to guide surgical approach. In testing on 50 frozen samples, correctly classified 45 (the model declined to recommend on 5 — appropriate refusal behavior for ambiguous cases)
- Shenzhen Institute of Advanced Technology's diffuse glioma classifier using whole-slide images, eliminating the need for molecular testing on standard cases
The pattern: high-stakes clinical decisions augmented by AI providing rapid second opinion, with explicit refusal pathways when the model is uncertain.
2. Hidden fracture detection
Fractures in difficult anatomical regions (wrist, hip, sternum) are commonly missed even by experienced radiologists. AI excels at finding subtle patterns hidden under soft tissues or in low-contrast images.
Reference deployments:
- Imagen's OsteoDetect — among the first FDA-cleared AI tools for clinical decision support (2018). Detects distal radius fractures in wrist scans. FDA clearance backed by performance data on 1,000 wrist images plus confirmation from 24 healthcare providers.
- YOLOv4-tiny applied to hip fracture detection: 95% accuracy, surpassing first-year medical residents and matching experienced radiologist performance.
The pattern: targeted AI for specific fracture types where missed diagnosis carries high clinical and legal cost. FDA pathway is established for similar tools, accelerating regulatory approval for new applications.
3. Breast cancer screening
Breast cancer is the second leading cause of death among American women. Routine screening misses up to 40% of breast lesions; conversely, ~90% of women with suspicious mammograms don't actually have cancer, leading to invasive followup procedures and patient anxiety. AI screening addresses both sides.
Reference deployment: Swedish study comparing AI-assisted screening to two-radiologist reading on women with average age 54. Each scan reviewed by both human radiologists and the AI tool. AI detected anomalies in 244 patients vs. 203 from radiologists. Of the 41 cases AI flagged that radiologists missed, 19 had invasive cancer. Critically, false-positive rate was identical (1.5%) between AI and radiologists — disproving the common assumption that AI screening generates more false alarms.
The pattern: AI as concurrent reader rather than replacement, validating against human performance metrics and demonstrating accuracy gains without false-positive trade-offs.
4. Neurological abnormality detection
Neurodegenerative disorders (Alzheimer's, Parkinson's, ALS) often present with subtle imaging signatures detectable years before clinical symptoms emerge. Earlier identification enables earlier intervention and patient planning.
Reference deployments:
- Retinal movement analysis for Alzheimer's, Parkinson's, ALS detection — 10-second analysis time, applicable in routine eye exams
- Speech pattern analysis for early Alzheimer's (patients with the disease tend to replace nouns with pronouns)
- Georgia State University TReNDS Center fMRI-based neurological disorder detection — model trained on fMRI data from 10,000 individuals, tested on 1,200 cases with known disorders. Detects Alzheimer's, schizophrenia, autism spectrum disorder via brain activity pattern analysis.
The pattern: AI identifying preclinical signatures across multiple modalities (imaging, behavioral, audio), with clinical follow-up to confirm diagnosis.
5. GenAI applications in radiology
Three production patterns emerging for generative AI in radiology workflows:
Image quality enhancement. Super-resolution GANs improve low-dose CT scan quality by 4× while preserving diagnostic detail. Reduces patient radiation exposure without compromising diagnostic accuracy. Image segmentation models highlight organs and abnormalities for radiologist review.
Radiology report generation. GenAI drafts initial reports from scan analysis. A research team's chest X-ray interpretation tool was trained on 900,000 medical images and reports, validated by radiologists who confirmed the model's first drafts contained no clinically significant inconsistencies, including life-threatening cases like pneumonia. Pattern: AI drafts, radiologist reviews and signs off.
Synthetic dataset generation. Cornell's RadImageGAN generates high-quality synthetic medical scans across 12 anatomical regions and 130 pathological classes, including annotations. Addresses the persistent training data scarcity problem in radiology AI development without privacy concerns or HIPAA exposure.
Five challenges to plan for
1. Development hurdles
Building production radiology AI requires curated medical imaging datasets — expensive to acquire, hard to label, often constrained by privacy regulations. Synthetic data and semi-supervised learning help, but quality medical labeling still requires medical expert time. Plan $50K+ for serious labeling work alone, more for cancer pathology, complex imaging modalities, or rare conditions.
2. UX integration
Radiology AI tools are only as effective as their integration with PACS (Picture Archiving and Communication Systems), RIS (Radiology Information Systems), and reporting workflows. AI that requires radiologists to switch between systems or learn new interfaces faces adoption resistance regardless of accuracy. The deployments that succeed integrate seamlessly into existing reading workflows.
3. Compelling business case identification
Radiology AI delivers measurable value, but identifying the highest-leverage workload requires data: which scan types have the highest miss rate, which procedures are throughput-limited, where do reading queues create patient-care delays. Without baseline data, ROI math is fiction.
4. Black-box outputs and explainability
Deep learning models that work but can't explain their reasoning don't pass clinical or regulatory review. Mitigation patterns: explainability layers (Grad-CAM, attention visualization for CV models), confidence scores with calibrated thresholds, refusal templates for ambiguous cases, structured uncertainty quantification, citation chains for any GenAI-generated findings.
5. Regulatory and ethical considerations
FDA SaMD pathway adds 12–24 months and $200K–$1M+ for diagnostic AI tools. International regulations (EU AI Act, MDR for medical devices, jurisdiction-specific privacy laws) compound this. Most early-stage radiology AI projects scope below the SaMD threshold (information-only output, not autonomous diagnosis) to avoid regulatory overhead while building toward eventual full clinical decision support.
Future of AI in radiology
Three developments shaping the next phase:
Multimodal radiology AI. Combining imaging with EHR data, lab results, genomics for integrated diagnosis. Already showing measurable accuracy gains on complex cases that single-modality tools miss.
Foundation models for radiology. HOPPR's Grace, Microsoft's MAI-DxO, and similar large-scale foundation models trained on medical imaging across modalities. These accelerate development of new applications without per-application training from scratch.
Continuous learning systems with regulatory approval pathway. The FDA's emerging framework for "Locked vs. Continuously Learning" AI in clinical settings will determine whether radiology AI can improve from production data without retraining and re-approval cycles.
The teams shipping ahead in radiology AI today are deploying disciplined narrow-task tools (specific cancer screening, specific fracture types, specific abnormality detection) and building toward integrated multimodal systems over the next 3–5 years. The competitive advantage compounds — each successful narrow deployment builds clinical trust and operational data for the next, broader deployment.
What's deployable today vs. pilot
Production-ready (FDA-cleared or equivalent):
- Targeted fracture detection (wrist, hip, ankle)
- Breast cancer screening as concurrent reader
- Lung nodule detection on CT
- Diabetic retinopathy screening
- Stroke triage on emergency CT
- Image quality enhancement for low-dose imaging
Pilot-stage / requires clinical validation:
- Multimodal diagnostic systems combining imaging + EHR + genomics
- Foundation-model-based radiology assistants
- GenAI report generation without per-finding sign-off
- Continuous-learning AI systems in clinical workflow
Wait:
- Fully autonomous radiology diagnosis without specialist review
- AI-driven treatment recommendations from imaging without multidisciplinary clinical review
- Cross-jurisdiction deployments where regulatory regimes conflict
The honest framing
AI radiology has moved past the proof-of-concept stage. The deployments shipping in 2026 are augmentation tools — second readers, screening accelerators, report drafters, image enhancers. Fully autonomous diagnostic AI is further out, gated by regulatory pathway and clinical validation requirements that take years to build.
The hospitals and radiology practices succeeding today are deploying narrow targeted tools, integrating them deeply into existing workflows, measuring outcomes against clear baselines, and scaling to additional applications based on validated results. The competitive advantage compounds — each successful AI deployment builds the clinical operations, integration patterns, and data foundation for the next.
Ready to scope an AI radiology project? Run the Project Estimator for a deterministic ballpark, or book a 45-minute Discovery with our healthcare AI engineers — we'll review your imaging modalities, integration requirements, and regulatory constraints and tell you honestly which applications are ready for clinical deployment.
Talk to the team behind this
Building something like this in production?
Our senior engineers ship this kind of work for real teams. 45-minute call, no pitch deck — just architecture, trade-offs, and whether we're the right fit for your problem.