Assessing the cost of implementing AI in healthcare
Honest engineering breakdown of healthcare AI cost in 2026 — six factors that drive the price, three real engagements, and the compliance overhead most projects underestimate.

Healthcare AI cost ranges aren't tidy. The honest spread for the AI components alone runs from $40K for narrow ML functionality bolted onto an existing system to $200K+ for a custom deep learning solution with full HIPAA compliance and SaMD pathway considerations. The spread between those numbers isn't waste — it reflects real differences in workload complexity, compliance load, and the architectural choices that determine whether the system can actually be deployed in clinical settings.
Six factors explain almost every cost gap we see between healthcare AI engagements. Three of those — compliance overhead, integration with EHR/EMR systems, and data acquisition under HIPAA — are where most healthcare AI projects underspend at scoping and overrun in delivery.
This article maps the cost structure, with three real JustSoftLab portfolio engagements as anchors. For broader healthcare positioning, see /industries/healthcare. For deeper treatment of the AI cost economics across industries, see calculating the cost of generative AI and how much does AI cost in 2026.
Six factors that move healthcare AI cost
1. Solution complexity and AI model type
Healthcare AI development requires a cross-functional team — data scientists, ML engineers, MLOps, healthcare-specific software engineers, QA, business analysts, project managers. AI projects also have a research component that regular software engineering doesn't: developers can't always tell upfront when the model will reach the required accuracy. With complex systems like autonomous AI agents, the timeline uncertainty alone moves the cost band substantially.
Model complexity drives a 5–10× cost spread:
- Static ML models (decision trees, classical classifiers): $30K–$50K. A decision-tree classifier predicting patient readmission lands in the lower half of this range.
- Deep learning models for clinical use cases: $60K–$150K. Cancer diagnosis assistance, treatment recommendation systems, medical imaging classifiers.
- Generative AI for medical imaging or structured generation: $150K–$500K+. GAN-based synthetic medical image generation, multimodal diagnostic systems, clinical Q&A with audit trails.
The right model isn't the most capable one — it's the one that solves the workload at acceptable accuracy. Most healthcare AI projects we see ship better outcomes with a simpler model and more data discipline than with a complex model and rushed data preparation.
2. Infrastructure: on-premises, cloud, or edge
Three deployment models, each with distinct cost structure:
| Dimension | On-premises | Cloud | Edge |
|---|---|---|---|
| Initial cost | Highest (hardware purchase) | Lowest (pay-as-you-go) | Moderate (deployment + cloud hybrid) |
| Recurring cost | Lowest (electricity + maintenance) | Highest (monthly fees scale with usage) | Mid (cloud for general data, edge for inference) |
| Scalability | Slow, capital-intensive | Fast, elastic | Mid (still need to scale endpoints) |
| Security responsibility | Full ownership | Shared with vendor | Shared, but data-in-transit risk reduced |
| HIPAA compliance | You're responsible for everything | Vendor offers BAA, but you still configure correctly | Combination — local data is your responsibility |
| Latency | Lowest (no network round-trip) | Variable (network-bound) | Lowest (local processing) |
Concrete cost ranges in 2026:
- Cloud inference for a simple AI model on standard CPU: $430–$650/month.
- Cloud training for a GAN-based or larger model on TPUs: $5K–$15K for the training run, plus ongoing inference.
- On-prem hardware for static ML: $5K baseline.
- On-prem GPU rig for deep learning: $20K–$50K for moderate setups.
- On-prem TPU/multi-GPU for GAN or large model: $100K+.
For HIPAA-bound workloads, the right answer is often a hybrid: cloud for training and general analytics where the cloud vendor's BAA gives clean compliance posture, edge or on-prem for inference where latency or data residency dominates.
3. Integration with existing systems
This is where most healthcare AI projects underestimate. Hospitals run dozens of legacy systems — EHR, EMR, PACS, lab information systems, billing platforms, scheduling, telemedicine. AI that doesn't integrate cleanly with these is a science project, not production software.
Realistic integration line items:
- EHR/EMR integration (Epic, Cerner, Athena): $8K–$25K per system, depending on whether the EHR vendor offers FHIR APIs or you're building bridges to legacy interfaces.
- Medical device middleware and APIs: $10K+ per device class.
- UI customization to fit clinician workflows: $10K+, often more if the AI output needs to integrate into existing report templates or imaging viewers.
- Legacy system reverse-engineering: $25K–$50K when proper documentation doesn't exist (which is more common than vendors admit).
The pattern: integration costs alone often equal AI model costs on healthcare projects. Plan for it explicitly during scoping. The "we'll figure out integration later" approach is the most common cost overrun trigger we see.
4. Implementation approach
Three paths, each with a clear cost-vs-customization trade-off:
Off-the-shelf AI models. Pre-built solutions (commercial NLP for medical records, image classifiers for radiology, validated decision-support tools). Initial cost is mostly integration ($10K–$50K) plus recurring licensing fees. Optional retraining on your data adds $10K+ for classical ML, more for LLM fine-tuning. Best for narrow workloads where commercial solutions already perform near-optimally.
Customized AI models. Existing AI architectures adapted for healthcare needs — fine-tuning a foundation model on medical text, customizing a CV model for specific imaging modalities. Initial cost: $50K+, scaling with customization depth and model complexity. The right path for most mid-size healthcare AI projects.
Built-from-scratch models. Designed specifically for the workload, owned entirely by the customer. Initial cost: $100K to $500K+ for cutting-edge applications. Higher upfront cost but no licensing fees and full IP ownership. The right path when the workload is unique enough that commercial tooling can't address it, or when regulatory pathway requires full provenance over the model.
For LLM-based applications, build-from-scratch is rarely the right answer — fine-tuning an existing foundation model is the practical path. See our LLM training stages article for the honest cost framing.
5. Data acquisition and training data availability
Medical data is scarce, expensive, and tightly regulated. The factors that drive data costs in healthcare AI:
Data collection. Internal hospital data is often sufficient for narrow models, but rarely for broader workloads. Commercial medical datasets cost $10K–$100K+ depending on type and exclusivity. Free depersonalized datasets exist (i2b2, MIMIC) but require approved research proposals. Synthetic data generation via GenAI is increasingly viable but requires manual verification by medical experts.
Data labeling. Medical expertise for annotation is expensive: $10K minimum for a basic project, $50K+ for cancer pathology, radiology, or clinical decision-making datasets. Generative AI labeling can speed up the work but still requires medical-expert validation, so the labor cost only partially shifts.
Data cleaning and preprocessing. $10K minimum, scaling with dataset size and complexity. Unstructured data (free-form clinical notes, scanned forms, multi-format imaging) compounds the cost.
Data sharing agreements. When your dataset isn't large enough on its own, partner agreements with other health systems or research institutions add legal and administrative overhead — typically $10K–$30K in setup.
The 30%-of-budget rule for data preparation in general AI is closer to 35–45% in healthcare, especially when the model targets a regulated clinical application.
6. Regulatory compliance
This is the line item most teams underestimate. Healthcare AI compliance overhead routinely adds 25–40% to total project cost.
HIPAA compliance. Authentication, secure connections, encryption at rest and in transit, audit logging, access controls. Certification costs alone run $10K–$150K depending on organization size, infrastructure, and current compliance posture. The engineering work to actually meet HIPAA requirements is typically twice the certification cost — encryption with customer-managed keys, role-based access on retrieval, audit logs that join model output to user identity and timestamp, breach notification systems.
FDA pathway considerations. If the AI is classified as Software as a Medical Device (SaMD) — for example, a diagnostic decision-support system — FDA 510(k) clearance or De Novo pathway adds 12–24 months and $200K–$1M+ in regulatory work. Most early-stage healthcare AI projects deliberately scope below the SaMD threshold (information-only, not diagnostic) to avoid this overhead.
HITRUST and SOC 2. Many healthcare customers require HITRUST or SOC 2 Type II from their vendors. Initial certification is $50K–$150K plus ongoing audit cost.
Clinical validation. Beyond regulatory compliance, real-world validation studies (compared to clinician baseline, on representative patient populations, with statistical power) are non-negotiable for clinical adoption. Plan $50K+ for a meaningful validation study, more for prospective trials.
For deeper treatment of compliance patterns in regulated AI workloads, see our reference architecture for fintech RAG — many of the same patterns (audit trails, citation tracking, RBAC, encryption) apply directly to healthcare with HIPAA-specific implementations.
Three real engagements
Project 1: AI-powered telemedicine analytics
A US-based healthcare technology company contracted us to upgrade their telehealth system with video analytics that surface communication patterns from recorded consultations. Goal: help clinicians improve patient interactions through measurable feedback.
The AI work. Two AI models. First, voice-to-text using NVIDIA NeMo's speech recognition for clinical-grade transcription. Second, emotion-sensitive analysis identifying seven emotion classes (anger, disgust, fear, happiness, sadness, surprise, neutral) using a deep transformer-based network for video and Wav2Vec 2.0 for audio. Both models were available off-the-shelf and fine-tuned on public datasets. We built the API integration into the client's existing telehealth workflow.
Cost: ~$160K for the AI components. The cost reflected the dual-model architecture, integration into a HIPAA-compliant telehealth platform, and validation work.
Project 2: Clinical decision support for cancer treatment
A healthcare analytics company partnered with us to build a clinical decision support platform that improves cancer prognosis accuracy and recommends personalized treatment options.
The AI work. A static AI model built from scratch, trained on a cancer research dataset from a US-based university partner. Clinically clean data — pre-organized, preprocessed, ready for training without significant data preparation overhead. The model takes patient demographic data, cancer type and stage, and proposed treatment options as input, and outputs a five-year prognosis per treatment option. We delivered a web interface for physicians plus report-building and visualization tooling that turns model output into clinical-grade reports.
Cost: $120K–$160K. Lower end of clinical-AI cost ranges because the dataset was clean and the workload was bounded — neither generative nor diagnostic-class (information-only output, not SaMD).
Project 3: ML-driven IOL power calculation platform
A laser eye surgery clinic developed a proprietary ML formula for calculating intraocular lens (IOL) power for patients with cataracts and other eye conditions. They commissioned us to build a web platform that runs their proprietary method and benchmarks it against established formulas.
The AI work. Two custom models built from scratch. A computer vision model that examines medical eye scans and extracts the relevant anatomical measurements. An ML model that takes those measurements and calculates IOL power using the client's formula. The CV model can also flag and correct measurements that fall outside expected ranges. Both were trained on the client's small initial dataset, with continued training on real-world data after deployment.
Cost: ~$100K for the dual-model build and training infrastructure.
These three engagements span the typical range. The pattern: simpler architectures + clean data + bounded compliance scope land in the $100K–$160K band; complex multi-model systems with full clinical integration push toward $200K+.
How AI reduces healthcare costs
The investment justifies itself when AI hits real workflow leverage points.
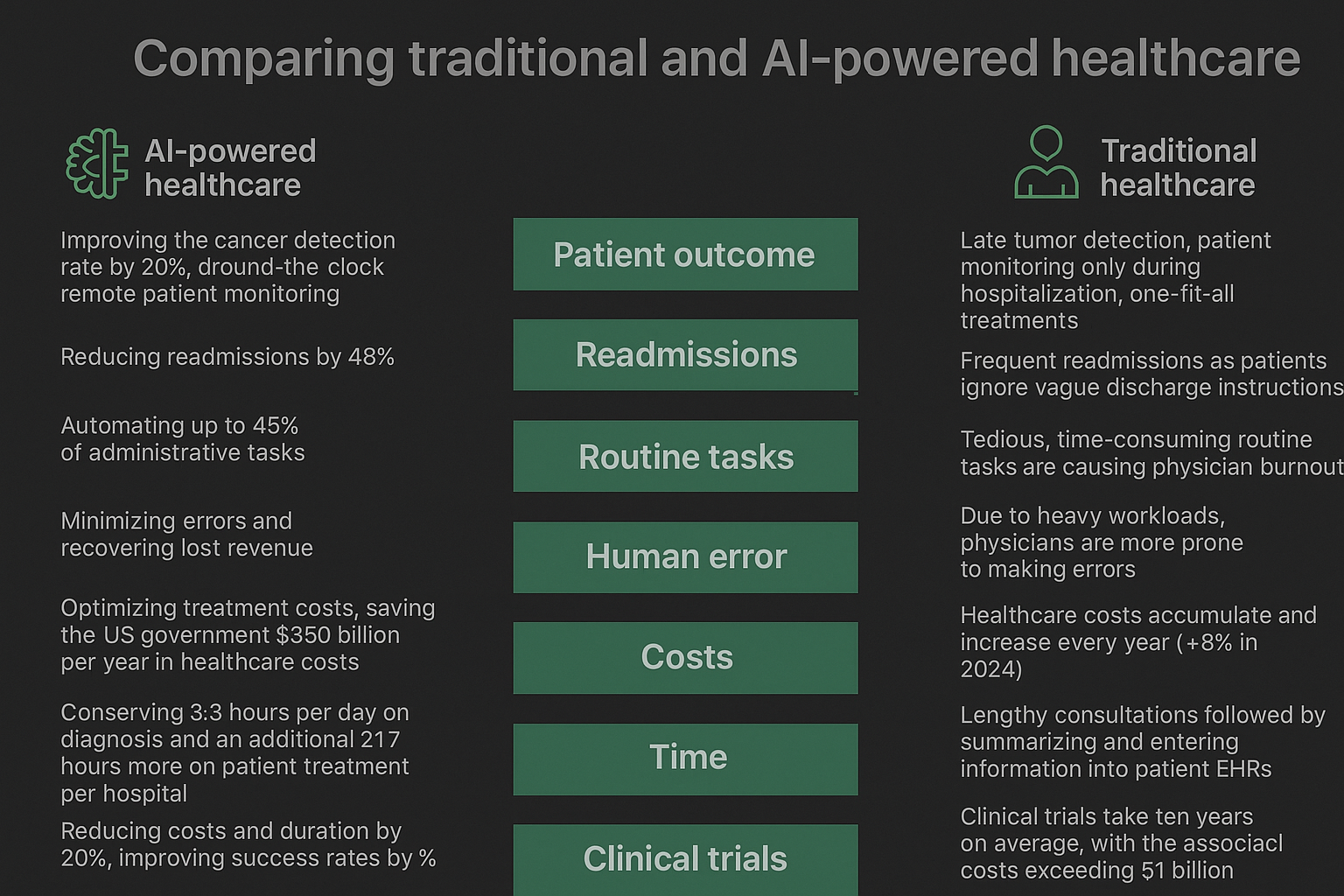
Diagnostic accuracy. Swedish breast cancer screening study: AI improved detection rates by 20%. Cancer treatment prognostic accuracy improvements of similar magnitude across multiple modalities. Better diagnosis cuts downstream cost (fewer late-stage treatments, fewer readmissions, better outcomes per dollar).
Readmission reduction. AI-driven mobile care plans for high-risk patients reduced readmissions by 48% in one published study. Readmissions cost roughly 10% more than initial admissions, plus regulatory penalties — readmission reduction is among the highest-leverage AI applications in hospital operations.
Administrative automation. McKinsey analysis suggests AI could automate up to 45% of administrative tasks in healthcare for $150B in annual US savings. Real revenue recovery: published case of $1.14M in revenue recovered from one organization through AI-driven coding error reduction.
Clinician time recovery. Medical imaging AI saves 3.3 hours of diagnostic time per radiologist per day, with cumulative time savings of 21+ hours per day per hospital across treatment workflows. The cumulative effect over a year is substantial — and it shows up in physician burnout reduction and patient throughput, not just direct labor cost.
Clinical trials. Generative AI in pharmaceutical R&D shows 10% trial success rate improvement and 20% reduction in cost and duration. Compounding effect across the drug development pipeline.
Payer-side optimization. McKinsey estimates AI-equipped payers can save 25% on administrative costs and 11% on medical expenses while seeing revenue growth.
The pattern: healthcare AI investments justify themselves on operational metrics that the C-suite already tracks (readmission rate, time-per-case, claim accuracy, trial success rate). Tying the AI investment to these metrics during scoping is what separates projects that get continued funding from projects that quietly die after pilot.
Is healthcare AI worth investing in?
Deloitte reports 94% of healthcare executives consider AI critical to their strategy. The consensus is real, but consensus doesn't fund individual projects — measurable ROI does.
The pragmatic path:
- Start with PoC. $20K–$40K, 4–8 weeks. Validates the workload, surfaces integration risks, lets you scope the full project on real data.
- Pilot at limited scope. A single workflow, single department, measurable KPIs. Six-figure investment that lets you demonstrate value before scaling.
- Scale only on validated outcomes. Don't expand scope based on enthusiasm — expand based on whether the pilot hit its KPIs.
If your organization has a data management foundation in place, AI initiatives cost dramatically less. If not, treat the data work as a prerequisite and do it deliberately, not as a side effect of the AI project. The teams that succeed in healthcare AI almost always sequence "data foundation → narrow AI pilot → scale" rather than trying to ship AI on top of broken data.
FAQs
How do infrastructure choices (cloud vs on-premises) affect healthcare AI costs? Infrastructure choice drives cost structure. On-prem requires $5K–$100K+ in upfront hardware investment, low recurring cost, and full HIPAA responsibility. Cloud is pay-as-you-go ($430–$650/month for simple workloads) with vendor-shared compliance posture. Edge AI balances local processing (low latency, reduced data-in-transit risk) with cloud for general storage. The right choice depends on data residency requirements, latency targets, and how much compliance work you want to own in-house vs. share with a vendor.
What are the hidden or ongoing costs of maintaining healthcare AI? Five places teams underestimate. Model retraining (15–20% of initial cost annually). Data drift monitoring and detection. Compliance audit cycles (especially for HITRUST and SOC 2 renewals). Security patching and incident response. Clinician training and workflow adaptation. None are exotic, but cumulatively they add 20–25% to year-2+ operating cost relative to a non-AI baseline.
How long does a typical healthcare AI project take? Plan in calendar quarters. PoC: 4–8 weeks. MVP: 12–24 weeks. Production deployment with HIPAA-compliant infrastructure: 24–52 weeks. SaMD pathway adds 12–24 months. Compliance review cycles routinely add 8–16 weeks to any phase. The realistic time-to-clinical-value for a serious healthcare AI project is 12–18 months from kickoff.
What's the cheapest way to test healthcare AI without committing to full project cost? A focused PoC on a narrow, low-risk workflow. Pick a use case with measurable KPIs, available data, and bounded integration surface. Spend $15K–$40K validating that the AI architecture works on your actual data. If the PoC succeeds, scale to MVP with confidence. If it fails, you learned at the cheapest possible price. The PoC discipline is what separates healthcare AI projects that ship from those that don't.
Ready to scope a healthcare AI project? Run the Project Estimator for a deterministic ballpark, or book a 45-minute Discovery with our healthcare AI engineers — we'll review your data, regulatory constraints, and integration surface and tell you honestly what's achievable in your timeline and budget.
Talk to the team behind this
Building something like this in production?
Our senior engineers ship this kind of work for real teams. 45-minute call, no pitch deck — just architecture, trade-offs, and whether we're the right fit for your problem.